Regeneration of Kidneys by Stem Cells
Kidney Regeneration
There are two types of kidney diseases – acute kidney disease and chronic kidney disease. In acute kidney disease (AKD) there is a rapid loss of kidney function. It occurs when there is a sudden major damage to kidneys. The principle causes are toxins and ischemia. While in chronic kidney disease (CKD), there is a progressive loss over kidney function. AKD is not detected at the initial stages and ultimately leads to CKD. The injuries are progressive in CKD and nephrons are also lost.
Adult stem cells derived from bone marrow might contribute to turnover and regeneration of several compartments of the kidney. Bone-marrow cells are known to migrate to the kidney and participate in normal tubular epithelial cell turnover and repair after acute kidney injury.
Podocytes (or visceral epithelial cells) are cells in the Bowman's capsule in the kidneys that wrap around the capillaries of the glomerulus. Podocytes are vitally important, and are also under enormous physical stress. It used to be thought that we were born with podocytes, and we die with the same podocytes — we don’t make any more during our lifetime. The only exception was certain rare types of kidney disease in which the podocytes abandon their blood-filtration duties to de-differentiate into less-specialized, dividing cells that little resemble their predecessors. As a result, the glomerulus collapses and the patients’ kidneys begin to fail. One such disease is HIV-associated nephropathy, or HIVAN. The role of a protein component of the telomerase complex called TERT was investigated. Although telomerase is best known as an enzyme involved in cell aging, recent research in lab have shown that TERT also plays a role in many types of cellular regeneration. Temporarily increasing the expression of TERT in adult, otherwise healthy laboratory mice caused the formerly stolid podocytes to abruptly de-differentiate and begin dividing. As a result, the glomerulus collapsed in a way that resembles what happens in humans with HIVAN. Conversely, ceasing the overexpression allowed the cells to stop dividing, re-specialize and resume their normal functions. Scientists looked closely at the glomeruli in humans with HIVAN, they found that TERT expression was increased. Equally important, the Wnt signaling pathway, which is important in embryonic development and in the self-renewal of stem cells, was also activated. Blocking Wnt signaling in a mouse model of HIVAN also stopped the podocytes from dividing and improved their function. The implication is that podocytes may utilize recognized pathways of regeneration to renew themselves throughout life. People suffering from chronic kidney disease may simply have worn out or outpaced their podocytes’ capacity for renewal. Now that the researchers know podocytes have the ability regenerate in response to common cellular signals, their next step is to learn whether this regeneration occurs in healthy animals and people. If this regeneration could be harnessed, one day people with chronic kidney disease could be treated.
http://med.stanford.edu/ism/2011/december/artandi.html
Kidney regeneration from ES cells
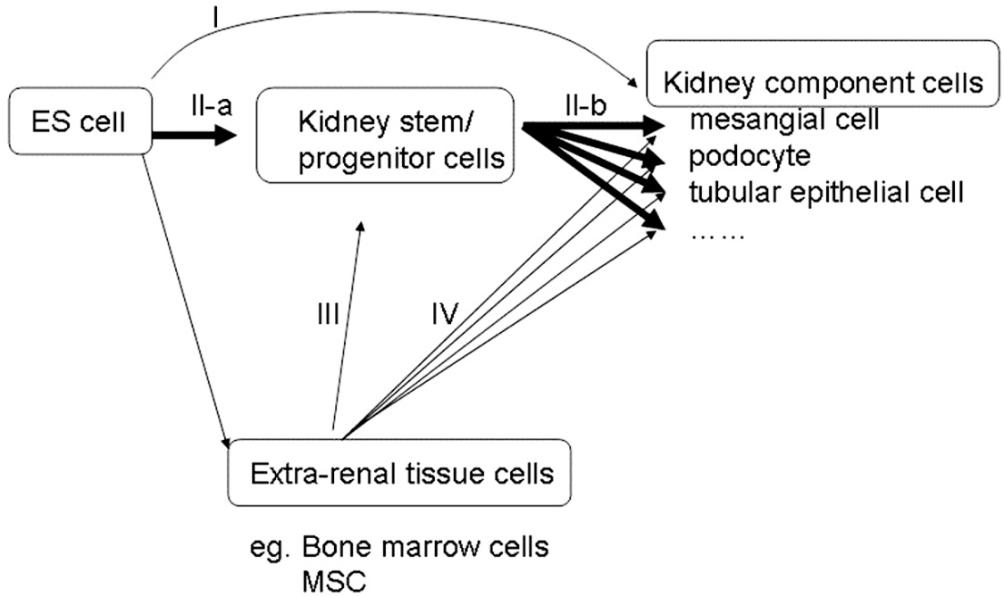
There are only few reports that show differentiation of ES cells into renal lineage. The concomitant use of retinoic acid, activin-A, and BMP-4 or BMP-7 induced the directed differentiation of human ES cells to renal precursors when analyzed by differentiation marker. As to the culture substrate, gelatin was reported to most closely recapitulate the directed developmental pattern of renal gene expression. The scientists radiolabeled human ES cells and transplanted it to fetal monkey kidney at the second trimester under ultrasound guidance and traced them by non-invasive imaging. A renal progenitor fraction of human ES cells was isolated. Serum concentration and feeder cell density was reduced to differentiate human ES cells. Differentiated cells were fractioned. These cells upregulated renal transcription factor compared to unfractioned cells.
In general, stem/progenitor cells and the proper microenvironment are essential for the repair or regeneration of damaged tissue. The same is true to the ES cell for the directed differentiation. A suitable microenvironment includes the presence of local cytokines as well as of extracellular matrix which can function as a scaffold and give rise to cytokines or growth factors around the stem/progenitor cell.
Kidney Regeneration from non ES cells
When bone marrow stem cells are co- cultured with ES cells, the phenomenon of cell fusion occurs. After cell fusion, ES cells can reprogram the cellular contents of bone marrow cells to adopt an ES cell phenotype.
Bone marrow-derived pluripotent MSCs have an ability to engraft to tubular epithelial cells in an experimental kidney injury model and to help to recover the lost renal function. It has recently been reported that kidney-derived MSC contribute to vasculogenesis, angiogenesis, and endothelial repair. This finding supports the possibility that MSC residing in kidney can participate in kidney repair or regeneration. But recent studies argue against the direct differentiation of bone marrow-derived stem cells or MSC into kidney. The relatively small frequency of engraftment of bone marrow-derived cells (3-22%) means that most of the kidney component cells are composed of kidney resident cells. Moreover the functional improvement in the recipient transplanted with stem/progenitor cells is not due to the existence of transplanted cell itself in the kidney. This may be due to the various cytokines secreted from transplanted MSC that organize an appropriate microenvironment for the kidney repair. To be sure, MSC secretes various cytokines such as VEGF, HGF and IGF-1. Injection of bone marrow-derived MSC into peritoneal cavity attenuated the cisplatin-induced renal failure without the engraftment of MSC in the kidney. The conditioned media from culture of these stromal cells induced migration and proliferation of kidney-derived epithelial cells and significantly diminished cisplatin-induced proximal tubule cell death. In considering the cell administration pathway, the finding from these two experiments indicates that it is the humoral factors, not cellular factors that contribute to the kidney repair or regeneration by MSC. Many factors have been proposed as candidates. One candidate is various cytokines secreted by MSC. Some of these factors are known to modulate kidney function or repair. For example, VEGF attenuates glomerular inflammation and accelerates glomerular capillary repair. HGF, an angiogenic growth factor, prevents epithelial cell death and enhances regeneration and remodeling of injured or fibrotic renal tissue. The effect of these growth factors or cytokines is evaluated as individual effect. Understanding the microenvironment in which the stem/progenitor cells is put in time and space in terms of cytokine expression would be firstly vital. This is the point from protein expression level.
Reference:
http://med.stanford.edu/ism/2011/december/artandi.html
http://en.wikipedia.org/wiki/Acute_kidney_injury
http://en.wikipedia.org/wiki/Chronic_kidney_disease
http://en.wikipedia.org/wiki/Podocyte
http://www.intechopen.com/books/stem-cells-in-clinic-and-research/regeneration-of-the-kidney-viewed-from-es-cell